HIGHLIGHTS
- We performed a systematic review and meta-analysis of TIPS effectiveness in Budd-Chiari syndrome with 17 studies that comprised 618 subjects.
- The pooled results (95%CI) showed a 19% (25.9–12.5%) rate of portosystemic pressure reduction.
- We found a 92% (83–97%) prevalence of living subjects five years after TIPS placement.
- Our study showed a 77% frequency (68–83%) of patients alive ten years after TIPS placement.
ABSTRACT – Background –
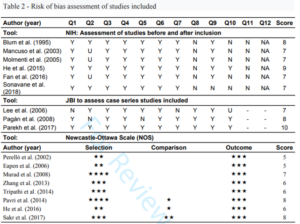
Budd-Chiari syndrome (BCS) results from the obstruction of the hepatic venous flow, usually at the level of the hepatic vein or inferior vena cava. When left untreated, it can progress with several complications, including liver cirrhosis. Transjugular intrahepatic portosystemic shunt (TIPS) appears to be effective in a subgroup of BCS patients. Objective – To perform a systematic review and metaanalysis of TIPS effectiveness in BCS treatment, considering the survival rate, reduction in portosystemic pressure, need for liver transplantation, technical failure, and shunt dysfunction for up to 10 years of follow-up. Methods – We evaluated 17 studies published in PubMed, Science Direct, Web of Science, and SCOPUS databases, which used TIPS as a treatment for BCS, comprising 618 subjects between 18 and 78 years old. We assessed the bias risk by the NOS, NHI, and JBI scales for cohort studies, before-after studies, and case series, respectively. We conducted the meta-analyses by extracting the number of events and the total patients evaluated to perform the proportion meta-analyses using the R software (“meta” package – version 4.9-6). Results – The pooled results (95%CI) showed a 19% (25.9–12.5%) rate of portosystemic pressure reduction, 6% (1–12%) rate for the need for liver transplants despite the use of TIPS, 2% (1–6%) technical failure rate, 30% (18–46%) shunt dysfunction rate, and 88% (81–93%) for the mean frequency of patients alive between 1 and 10 years after the procedure. We stratified survival rate and found an 86% (74–93%) prevalence of living subjects during less than five years, 92% (83–97%) at five years, and a 77% frequency (68–83%) of patients alive ten years after the TIPS placement. Conclusion – TIPS is an effective treatment for BCS, providing a high 10-year frequency of living patients and a significant decrease in portosystemic pressure. The need for liver transplants after TIPS and the technical failure rate is low.
AUTORES
Mariana Oliveira Amarante MORENO1, Cláudio Luiz da Silva Lima PAZ2, Maria Gabriela Fernandes DEZAN1,3,4, Lourianne Nascimento CAVALCANTE3,4,5 and Andre Castro LYRA3,4