HIGHLIGHTS
- It is well-known that endoscopic classification severity is a good predictor of the risk for strictures and the need for endoscopic dilatation after alkali ingestions.
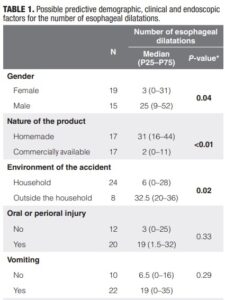
- We found that accidents with homemade products and accidents occurring outside the household environment were significantly associated with a greater number of esophageal dilatations in the longterm follow-up of children following alkali ingestion.
ABSTRACT – Background –
Children who experience alkaline injury are at risk for the development of esophageal strictures and the need for esophageal dilations. Objective – We aimed to assess predictors for a higher number of esophageal dilatations in children following alkali ingestion. Methods – Single-center retrospective cohort study including children who underwent esophagogastroduodenoscopy (EGD) after alkali ingestion. Possible predictive factors for the need for esophageal dilatations were evaluated. Results – A total of 34 patients were included, and 19 were female (55.9%). The median age at the time of the accidents was 20.6 months (IQR 15–30.7). All alkali ingestions were accidental, in all cases involving liquid products, and most (24/34; 70%) occurred at the child’s home. Homemade liquid soap was the agent in half of the cases. The most frequently reported symptom at presentation was vomiting (22/34, 64.7%). The median follow-up time was 3.2 years (IQR 1.1–7.4). On follow-up, the median number of esophageal dilatations required for these patients was 12.5 (IQR 0–34). Among demographic factors, male gender (P=0.04), ingestion of homemade products (P<0.01), and accidents happening outside of the household environment (P=0.02) were associated with a greater number of esophageal dilations on follow-up. An endoscopic classification Zargar of 2B or higher (P=0.03), the presence of stricture at the time of the second EGD (P=0.01), and gastroesophageal reflux disease (GERD) as a late complication (P=0.01) were also associated with a greater number of esophageal dilations on long term follow-up. Conclusion – Beyond the endoscopic classification severity – a well-known risk factor for the strictures after alkali ingestions, we found that male gender, accidents with homemade products, and accidents occurring outside the household environment were significantly associated with a greater number of esophageal dilatations in the long-term follow-up of children following alkali ingestion. Keywords – Caustic ingestion; alkali ingestion; endoscopy, child, esophageal dilations.
AUTORES
Annie J CARDOSO1, Natascha S SANDY2, Gabriela S GOMEZ1, Maria de Fatima SERVIDONI1, Elizete A LOMAZI1 and Maria Angela BELLOMO-BRANDAO1